
Anal vein thrombosis
"External haemorrhoids"
Painful haemorrhoid out of the blue
If you feel a - usually - painful lump at the anus, which is bluish in colour and has developed overnight, you may think of a haemorrhoidal condition. However, another condition is also a possibility: the reason for your discomfort could be anal thrombosis. But don't worry, unlike deep vein thrombosis (DVT), this vascular blockage is not threatening because the clotted blood cannot be washed into other vessels (embolism). In many cases, treatment is not even necessary and waiting and observing may already be the best therapy.
Read also the interview by Bild der Frau reporter Gabriele Eisenrieder with Dr Hofer.
Cause Analthrombosis: There are many triggers
In the subcutis around the anus there is a network of fine veins (plexus haemorrhoidalis externus). The name is misleading, these vessels have nothing to do with the real (internal) haemorrhoids. They divert oxygen-poor (dark red to blue) blood via the iliac vein (V. iliaca interna) into the inferior vena cava, which leads through the abdomen and thorax to the heart.
Even under normal conditions, blood flows in these vessels at a low pressure of about 15 mm Hg. Any compression or increase in pressure in the abdomen causes the blood flow in one of these vessels to stop. The vessel swells and the blood it contains clots - anal vein thrombosis has developed.

Other triggering factors are
- dilated vessels due to abundant alcohol consumption: at Oktoberfest time we see significantly more anal thromboses than in the rest of the year
- mechanical irritation (anal sex)
- Proctological operations
- Sclerotherapy or ligation of haemorrhoids
- Very rarely general illness with altered blood clotting tendency
"Haemorrhoid" in pregnancy and after birth
Pregnancy combines several risk factors: Hormonal changes lead to constipation in many women. The baby and amniotic fluid put pressure on the intestines and the pelvic floor. The body's water content increases steadily towards the delivery date, and the connective tissue becomes more stretchy. The general tendency to thrombosis also increases.
When pushing during birth, the pressure in the anal veins increases again. The passage of the baby leads to tears in the pelvic floor muscles, the resulting bruise sags to the lowest point. In postpartum women it is therefore not uncommon to find swelling around the anus, sometimes considerable ("cauliflower-like"), which is misunderstood as 4th degree haemorrhoids. Clinically, a mixed picture of anal thrombosis, swelling due to water retention (oedema) and haematoma is seen.

Symptoms Anal Venous Thrombosis: Pain & Itching
Some patients report non-specific precursors of symptoms (prodromes) one to two days before the onset of anal thrombosis, such as mild itching or tingling. Anal thrombosis manifests itself as sudden pain and a palpable bulge at the edge of the anus. Burning and stinging are also possible symptoms.
Anal vein thrombosis can be recognised by a bluish-black lump covered with shiny stretched skin. This feature helps the doctor diagnose anal venous thrombosis and rule out other conditions such as haemorrhoidal disease: The surface of haemorrhoids has the slightly granular or velvety texture of the transitional or intestinal mucosa. On simple palpation, a bulging, smooth-bordered lump that is displaceable relative to the surrounding area can be felt.
The size of an anal vein thrombosis can range from pinhead to plum-sized. Not infrequently one finds not only one, but several knots.
Good medical care consists in doing nothing as much as possible. (Samuel Shem 1978, The House of God)
The best treatment for anal thrombosis: Do nothing!
The good news is that anal venous thrombosis often heals on its own within a few days to weeks. So the essential part of treatment is to take away the pain until the body has healed itself. Furthermore, there are some tips to keep in mind so that the thrombosis knot does not expand any further. And last but not least, the diagnosis must be confirmed before you sit back and wait.
Pain therapy
- Common painkillers such as ibuprofen or metamizole (Novalgin®, Novaminsulfon ®) in tablet form often help best in the acute phase.
- Local anaesthetic creams such as Haenal akut Creme® or Posterisan akut Creme®, available without prescription from pharmacies, can be applied externally.
- Some patients find cooling pleasant and pain-relieving.
- Even on a busy day at work, you should take every opportunity to have a short lie-down.
- In the acute phase, one would also prefer to avoid strenuous sport.
Promote decongestion
- Anal thrombosis has little to do with inflammation. Nevertheless, anti-inflammatory ointments with cortisone often help to reduce the swelling of the tissue, probably through a membrane-stabilising effect.
- Heparin ointments are often used to prevent the growth of the blood clot (thrombus). The use of heparin injections or blood-thinning medications in this indication would not be recommended because the risk-benefit ratio has not been studied.
- The dissolution and resorption of the clotted blood can be promoted by gentle heat.
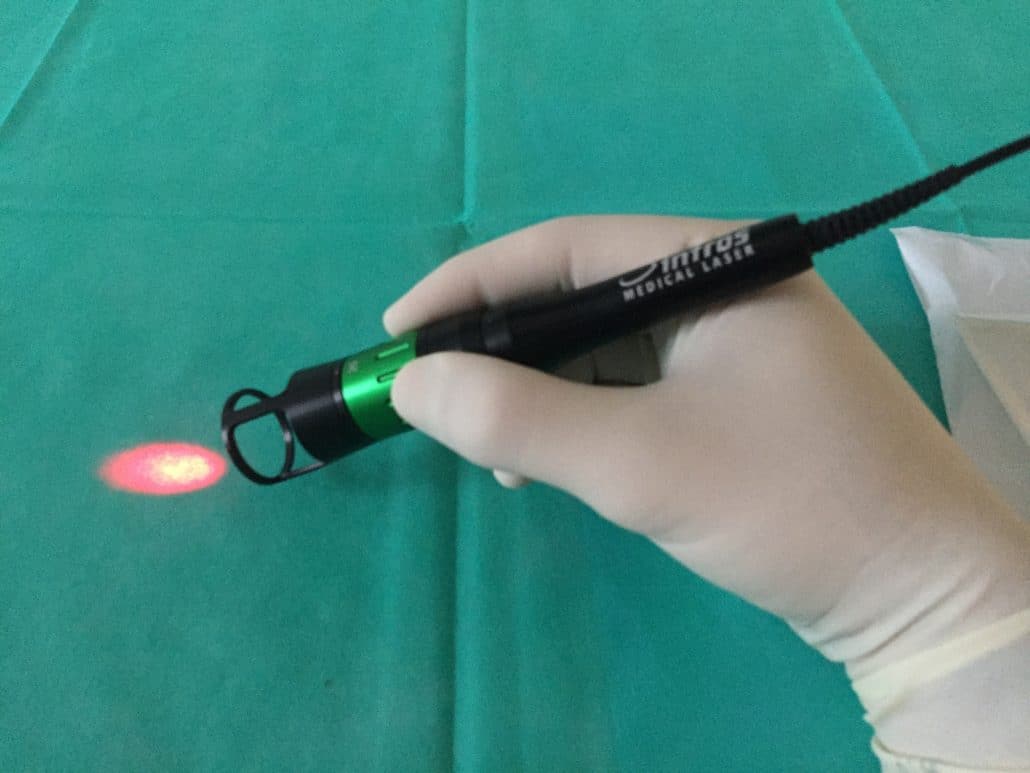
- Low Level Laser Therapy (LLLT) has an analgesic and resorptive effect.
Interventions and operations for anal thrombosis
Cutting open and squeezing out the clotted blood (coagulation) or surgical removal of the entire lump is often recommended. With the former method, the lump often fills up within hours; with the latter, a wound remains that takes a long time to heal. We would therefore only consider both measures in the case of extreme pain that cannot be influenced in any other way or if there is no regression over several weeks.
Sclerotherapy of internal haemorrhoids is also commonly practised, but is likely to have very limited effect on the swelling condition of anal thrombosis.
Anal thrombosis: Can complications occur?
Sometimes, however, the skin stretching over the thrombosis will be so stressed by the pressure that it opens and deflates on its own (spontaneous perforation). Supposedly, a persistent bleeding occurs. However, this is only the leakage of the blood that liquefies again, which stops by itself after a few days and is not dangerous. A commercial panty liner for these few days is the solution to the problem.
Although the thought suggests itself, a bacterial infection via this wound is quite unlikely. As mentioned above, the thrombus is fixed in the branched venous plexus, so that detachment and embolism do not occur. Also, anal thrombosis is generally not a sign to look for a coagulation disorder.
Anal thrombosis: Prevention
Some tips for prevention can be derived directly from the causes mentioned:
- Stool regulation, for example with psyllium husks
- Balancing breathing technique during sports and heavy lifting
- Breaks and exercise during long car journeys or long-distance flights
- Avoid excessive alcohol consumption
Bibliography anal thrombosis
Brearley, R. (1988). Perianal thrombosis. Diseases of the Colon & Rectum, 31(5), 403-404-403.
Delaini GG, Bortolasi L, Falezza G, Barbosa A. Trombosi emorroidaria ed ematoma perianale: diagnosi e trattamento [Hemorrhoidal thrombosis and perianal hematoma: diagnosis and treatment]. Ann Ital Chir. 1995 Nov-Dec;66(6):783-5. Italian. PMID: 8712590.
Eso Y, Yoshiji S, Nakakubo Y, Matsuura M, Seno H. Acute Anorectal Thrombophlebitis Caused by a Protein C Deficiency. Intern Med. 2018 Jan 15;57(2):209-212.
Grundei, T. (2015). Everyday proctology from a surgeon's perspective. Der Hautarzt, 66(6), 423-429.
Hager T. (1978). Frequent anal and perianal disorders and their treatment. Fortschritte der Medizin, 96(32), 1584-1588.
Hegde, R., Trombold, J. M., & Dominguez, J. M. (2020). Colorectal surgery review for primary care providers. Missouri medicine, 117(2), 154-158.
Herold A. (2020). Differenzialdiagnose des Hämorrhoidalleidens [Differential diagnosis of hemorrhoidal disease]. Der Hautarzt; Zeitschrift fur Dermatologie, Venerologie, und verwandte Gebiete, 71(4), 269-274.
Iseli A. (1991). Office treatment of haemorrhoids and perianal haematoma. Australian family physician, 20(3), 284-290.
Khalil, P. N., Kleespies, A., & Siebeck, M. (2009). Anal venous thrombosis [Anal venous thrombosis]. MMW Advances in Medicine, 151(39), 39.
Klug, W., & Knoch, H. G. (1984). Haemorrhoids and perianal thrombosis-diagnosis, therapy, results]. Zeitschrift fur arztliche Fortbildung, 78(7), 263-267.
Roblick, M., & Farke, S. (2018). Anal pain - emergencies in proctology. coloproctology, 40(6), 463-473.
Wienert, V., & Grubbendorf, E. I. (1973). Perianal thrombosis [Perianal thrombosis]. Fortschritte der Medizin, 91(29), 1137-1139.
DR. BERNHARD HOFER, FLORIAN LIEBL & COLLEAGUES
Specialists in surgery, proctology
Brienner Str. 13, D-80333 Munich, Germany
- info@darmsprechstunde.de
- 0049-89-292679
- Monday - Thursday: 08.00 - 13.00 and 14.00 - 18.00
- Friday 08.00 - 13.00
- Saturday - Sunday : closed
To protect your personal data, the connection to Google Maps has been blocked.
Click on Load map to unblock Google Maps.
By loading the map, you accept the privacy policy of Google Maps.
You can find more information about the privacy policy of Google Maps here Google - Privacy Policy & Terms of Use.
© 2021 Proctology Clinic Munich