Coccygeal fistula (pilonidal sinus)
All information for a good therapy decision
Quickly fit again for work and leisure
Coccygeal fistula -What to do?
People don't like to talk about health complaints when they affect sensitive areas such as the buttock crease (rima ani) or coccyx region.
With symptoms that are often nonspecific, you may have suspected a bruise, increased sweating, a persistent "pimple" or an uncomfortable bike seat as the cause.
Maybe you have already tried various methods to get rid of pain, induration or secretions of blood or pus, but without success. Maybe you have even had surgery and are tired of complex procedures with large skin incisions, uncomfortable tamponades and lengthy wound treatment.
Imagine a treatment that does not require hospitalization or large open wounds, yet removes the fistula without false compromises? A treatment with over 90% success rate.
Since the foundation of our practice in Munich, our specialists Dr. Bernhard Hofer and Florian Liebl have treated over 6000 patients with sinus pilonidalis. Since 2004, Dr. Bernhard Hofer has developed his minimally invasive technique of sinusectomy and laser ablation, based on the revolutionary idea of pit picking by Lord and Bascom.
Visceral surgeon Florian Liebl ideally enriches our spectrum with his extensive experience in reconstructive techniques (especially the Karydakis operation), which he acquired as a student of Prof. I. Iesalnieks.
Thus, we can now offer a promising therapy concept for almost every form of coccygeal fistula.
What is a fistula?
A fistula is a tubular duct formed as a result of chronic inflammation. There are fistulas in the area of the buttock fold as a result of penetrated hair(coccyx fistula), at the anus starting from the anal glands (analfistula) and in acne inversa (armpits, groin, buttock fold, anal region), a disease that occurs almost exclusively in smokers as a result of a pathologically altered immune reaction.
Emergency? Severe pain?
Then use this button to contact us for quick help! (Unfortunately we can only answer during office hours)
Need more information?
You want to know more? Here you will find the concentrated knowledge on coccygeal fistula:
Do I have a coccygeal fistula?
The 6-point checklistfor easy self-diagnosis
If you have these symptoms, you should think of a coccygeal fistula:
- Palpable induration or visible "bump" over the coccyx
- pain or feeling of pressure while sitting
- "Pimple" or "boil on the buttocks" on the side of the buttock crease that does not want to heal
These complaints indicate an abscess (accumulation of pus):
- Visible redness
- Rapidly increasing swelling
This practically proves the diagnosis of coccygeal fistula:
- Small openings or black dots in the centre line ("pits")
Cause and origin
How does acoccygeal fistula?
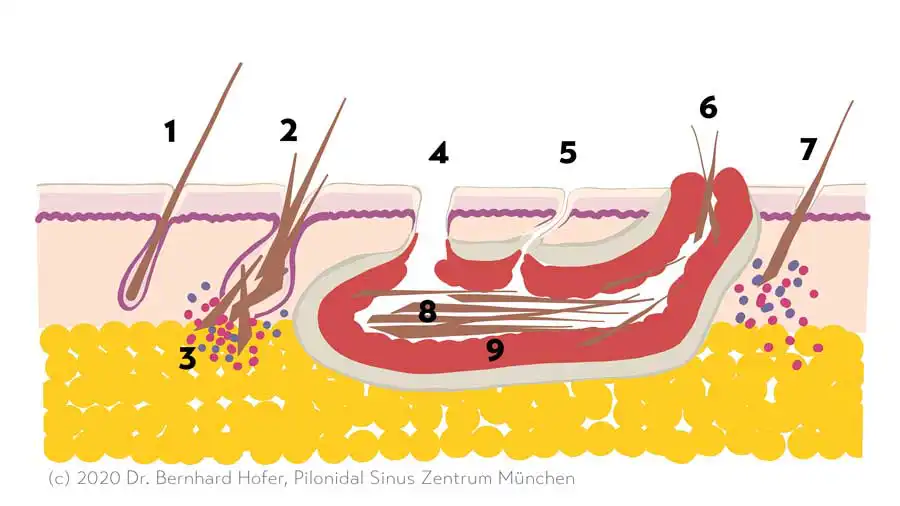
The Latin term "hair nest pit" (from Latin pilus 'hair' and nidus 'nest') best describes the problem. A pilonidal sinus is a collection of "ingrown" hairs - actually broken off and impaled in the hair root - in an encapsulated cavity, leading to inflammation of the soft tissues in the area of the buttock fold.
According to recent studies, hair from the head, especially freshly cut hair, can also bore into the intact skin of the gluteal fold and cause a fistula. This affects approximately 20% of patients with pilonidal sinus. Even more rarely, primary hair malformation occurs in the hair root and leads to keratin deposition in the hair follicle.
The opening of the hair root ("pore") widens and becomes visible, sometimes only as a tiny black dot. These openings are called "pit" or "porus" and allow the penetration of bacteria.
The pilonidal sinus has nothing to do with the coccyx bone or a developmental malformation ("dermoid cyst, sacral dermoid").
If you want to know more, you can continue reading on our Pilonidal Sinus Center page.
Where can I find help?
To which doctorfor pilonidal sinus?
A coccygeal fistula is a disease of the skin and skin appendages (the hair roots). The dermatologist will nevertheless refer you to the surgeon in most cases. Although surgery for a coccygeal fistula is performed at least 40,000 times a year in Germany, it is still a rare procedure in relation to the total population.
So you will only find a fistula surgeon experienced in minimally invasive techniques in specialised centres. You should see an expert because complications and recurrences are common.
Don't be afraid to ask your doctor which surgical technique he uses, what alternatives he sees and how often he performs the procedure per year.
In addition, the question of whether you need inpatient treatment in hospital and general anaesthesia is justified according to the expected healing time and the personal success rate of a surgeon.

Surgery for coccygeal fistula
0
Treatment cases
0
Years of pit picking experience
0
Years of laser experience
0
I am so thankful for Dr. Hofer and his team to provide the necessary procedure for my annual fissure that I had been suffering with for 18 months. The laser fissurectomy was relatively easy through out patient care. After the procedure I was fully recovered within a...
Read More "

I would like to express my deepest gratitude to Dr.Hofer and his medical practice.
I have suffered for many years, undergone extensive and unsuccessful surgeries and have been offered another butcher method surgery before I was lucky to find Dr.Hofer's practice.
My experience at the practice has been very friendly and pleasant....
Read More "

Very high recommendation for Dr. Florian Liebl, I visited him several times and he took such good care of me , he as well did surgery for me, I'm more than happy and grateful to have doctor like him. Very professional, caring, know his job, and he really gives him...
Read More "

I had a pilonidal cyst and I had the laser operation. I'm from France, so it's quite a distance but it's worth it, after 2 months I don't feel any pain and I'm now cured!
It's easy to communicate even if you don't understand German, the doctor has a translation solution.
The...
Read More "

I could live a thousand years and not outlast my gratitude towards Dr Hofer and his practice. In January, I traveled to Germany from Toronto for a procedure that is not offered anywhere in Canada. For years, I lived in despair, dealing with unimaginable agony and no relief. Local doctors...
Read More "

Gain time to think ...
Coccygeal fistula - treatmentWithout surgery
The first two questions asked after a diagnosis of coccygeal fistula are always, "Does the fistula need surgery?" and "Is there a treatment option without surgery?"
If you want to get rid of your coccygeal fistula, there is no way around surgery. On the other hand, a pilonidal sinus is not a life-threatening condition. Complications such as blood poisoning (sepsis) or the development of a malignant tumor are rare to extremely rare. The development of a coccygeal fistula usually occurred a long time ago when it is diagnosed. Significant enlargement occurs very slowly, if at all. However, you do not have to permanently accept the symptoms such as bleeding, pus discharge, unpleasant odor and variable pain. If there are no symptoms (asymptomatic, "bland" form), you can also wait.
What then is the value of conservative treatment measures at all?
A less severe inflammation can be treated temporarily with antibiotics. However, this does not make the fistula disappear. Traction ointments may possibly promote spontaneous opening of an abscess, but the benefit of these products has not been proven.
Regular shaving and removal of visible loose hair can prevent additional hair from entering the fistula tract and relieve symptoms. Good hygiene, including daily showering of the buttock crease once or twice a day, reduces the density of bacteria on the skin. Antiseptic ointments with iodine or chlorhexidine also have this effect.
With these tips, you can keep the level of inflammation as low as possible and buy time to schedule the procedure at the best possible time and under the best possible conditions. It is rarely necessary to cancel a vacation or postpone an exam because of a diagnosis of coccygeal fistula.
Keep your nerve, choose the smallest possible intervention!
Acute treatmentfor pilonidal abscess
Acute inflammation is often the first sign of pilonidal sinus. It is often preceded by prolonged periods of sitting, such as during exam preparation, urgent office projects, or after a long-haul flight. A bruise during sports or a fall are also frequently cited as possible triggers. The fistula tract fills with pus, the swelling increases rapidly within a few days, and the pain can be unbearable. This is called a coccyx abscess.
At this stage, treatment should focus on eliminating the inflammation. This is best achieved by opening through a small incision under local anesthesia. Ultrasound examination helps to select the optimal site for the procedure. Afterwards, the patient should be free of symptoms within one to two days. The treatment of the fistula can be planned without time pressure. Complete excision in the acute situation is not recommended (in accordance with the guidelines).
General symptoms of illness such as fever or severe circulatory reactions in the context of sepsis are extremely rare.
In the early stages of inflammation or when surgical opening is not possible, antibiotic therapy may possibly be sufficient.

First think, then cut ...
Operationsfor chronic coccygeal fistula
Radical surgery with open wound treatment
The clinical picture of pilonidal sinus was first described by Herbert Mayo in 1833 and was given its name by Hodges in 1880. Until the middle of the 20th century, the prevailing opinion was that pilonidal sinus was a congenital clinical picture. The large number of recurrences of the disease (relapse) after surgical removal led to the concept of "radical excision" (from the Latin radix = root) of ever greater extent.
It is now recognised that it is an acquired condition caused by hair. However, the majority of surgeons worldwide still believe that the best treatment is a large-scale excision, leaving a safe distance of healthy tissue down to the coccyx.
In this process, the surgical wound is left open. Gradually the wound is supposed to fill with scar tissue and thus healing is achieved. The healing process is long and prone to disturbances. We see quite a few patients who do not reach a stable state of healing even after months to years. Elaborate and sometimes painful wound treatments put a strain on the patient. Absences from school, training and work often impair professional development.
Simple closure by suturing in the midline is rarely successful. Wound healing disorders and infections are the rule rather than the exception, so that sutures have to be removed again prematurely or a scar that has just healed bursts open again.
We therefore advise against this procedure, which is also described in the Guideline Coccygeal Fistula recommended in the guideline on coccygeal fistula.
Radical surgery with plastic closure
Therefore, various techniques have been developed to achieve a stable suture through a so-called plastic closure. Under a flap plastic surgery means the closure of a defect by tissue taken from another part of the body, not the use of plastic. For coccygeal fistula, the Karydakis plastic, the cleft lift operation according to Bascom and the Limberg plastic are mainly used. Even these complex surgical techniques cannot guarantee a permanent cure and have their specific complication possibilities. If performed correctly by an experienced surgeon, the Karydakis operation in particular is a good solution if other techniques have not led to success.
Gentle surgical techniques: Pit picking and its variants
The pit-picking technique was developed by Peter Lord in London in 1965. However, it only became more widespread through John Bascom from Oregon, U.S.A. The basic principle consists of removing the entry ports (ingrown hair roots, "pits") and freeing the fistula tract from hair and inflammatory material. In this originally described technique, the fistula capsule is left in place. With this variant, healing rates of up to 70 % are achieved. To improve these results even further, methods have been developed to remove the fistula tract completely without making a large incision (synonyms: minimal tubular fistula excision, fistulectomy, sinusectomy), which increases the healing rates up to 90 %. Another approach is to burn out the fistula tract with a special laser probe. This principle, originally introduced for the treatment of anal fistulas, is called FiLaC (Fistula Laser Closure) or SiLaC® (Sinus Pilonidalis Treatment), up to 80 % of the fistulas treated in this way heal.
All these variants of the pit-picking technique have their justification. We make the decision about the respective procedure on the one hand depending on the type and extent of the fistula. It also plays a role whether the preference of the patient is more on the fastest possible healing or more on the sustainability of the restoration.
If another operation has not led to success, the principles of pit-picking can also be applied in the relapse situation. In our practice, about 30% of patients with pilonidal sinus have already undergone conventional surgery one or more times. There is almost always a method of treatment that can avoid further downtime due to a painful wound.
Treatment procedure at the Pilonidal Sinus Centre Munich'
We perform almost all operations under local anaesthesia (local anaesthesia) and on an outpatient basis with little strain on the organism. With the use of diluted local anaesthetic (the tumescent anaesthetic known from aesthetic surgery), even major operations can be carried out completely painlessly and safely. The advantage of these anaesthetic methods is also that pain-free sitting on the drive home is possible even after the procedure. The local anaesthetic also has a germicidal (bactericidal) effect and thus helps to prevent infections.
We have summarised the exact treatment procedure for the removal of a pilonidal sinus in the Pilonidalsinus Zentrum München on the page Treatment procedure and the information sheet Outpatient surgery and treatment of a pilonidal sinus (pilonidal sinus).
{kind=link}
All right?
FAQ - Frequently asked questions about coccygeal fistula surgery
Provided the diagnosis is correct, treatment of coccygeal fistula is almost always possible with our minimally invasive methods. You are welcome to send me your history and picture documentation via the contact form, then we can say more about the individual case.
No, today we actually no longer see a reason for radical surgery in any case. We supplement the conventional pit-picking with a peeling out of the fistula capsule ("fistulectomy") or, less frequently, with a laser treatment ("FilaC") and are successful with this in about 90 % of cases, even if pit-picking operations have already taken place in the past.
Yes! Very often a recurrence of a coccygeal fistula (recurrence of a pilonidal sinus) is caused by hair roots that have grown in again or penetration of hair into the still sensitive scar. In the former case, pit-picking, in the latter, laser hair removal and release of invaded hairs leads to permanent healing. If this strategy is not applicable, we will advise you on the proven alternative of Karydakis or Cleft Lift surgery.
The operation itself is a benefit of the statutory health insurance. We are approved for treatment by all statutory health insurance funds. A number of health insurance companies have even concluded special care contracts with us for the treatment of coccygeal fistula. Many patients also choose a treatment for permanent hair removal as a preventive measure, which is not paid for by most health insurance companies and costs € 70 per treatment with us.
Depending on the complexity of the fistula and necessary consumables (laser probes), they invest between 600 and 1200 € for outpatient treatment under local anaesthesia.
More than 95 % of the procedures we perform are carried out under local anaesthesia without any problems or pain. The patient can return home after a short period of monitoring. If the patient has to travel a long way, it is possible to stay overnight in a hotel in Munich after the operation. If preferred, the operation can be performed under general anaesthesia in the Iatros Clinic. For an additional charge, an overnight stay in the Iatros Clinic is also possible. However, the laser for hair removal is not available at the clinic.
In this situation, we first carry out a pre-treatment with puncture of the abscess and/or antibiotics. The inflammation subsides and the actual fistula operation can take place about 1 - 2 weeks later.
Simply fill out the contact form above and upload 1 - 2 meaningful pictures of the findings. One of our doctors will then contact you and send you a proposed appointment. You are welcome to give us a time window for the desired appointment.
I have a long way to travel, is it possible to schedule the examination and surgery on the same day?
Yes, this is possible. If it is your express wish, you can waive your right to a cooling-off period and a second opinion, and the procedure can follow directly after the examination. Please inform us of this wish when making your appointment so that we can calculate sufficient time! This option is taken by the majority of patients. If you are not yet sure about your decision, we will be happy to arrange a second appointment for the treatment.
The duration of the inability to work depends very much on the type of surgery performed. After conventional radical surgery, it is not uncommon to have a large wound that makes sitting and walking very difficult. Frequent dressing changes and wound treatments are also usually necessary. In these cases, the patient may be unable to work for at least 4 weeks, but also up to months. This is the great advantage of the minimally invasive surgical technique. With us, hardly any patient is off sick for longer than 2 weeks. Any kind of physical activity is permitted again from the 2nd day after the operation.